Donnie Yance is an internationally known master herbalist and nutritionist. He is the author of the book, "Herbal Medicine, Healing and Cancer" and "Adaptogens in Medical Herbalism"
As a musician and composer, I’ve always been fascinated by the power of sound. We know sound waves can shatter glass, create beautiful music, and even help babies develop in the womb. But what if I told you that precisely controlled sound waves could also destroy cancer cells while leaving surrounding healthy tissue completely untouched?
This isn’t science fiction, it’s a revolutionary medical treatment called histotripsy. Think of it as ultra-precise microsurgery, but without a single incision. No scalpels. No radiation. Just carefully focused sound waves that work with remarkable precision.
Traditional Herbal Medicine (THM) is very different from using isolated plant compounds. Using isolates to treat cancer is a more allopathic approach and not at all part of a holistic whole-systems model based in THM practice.
THM is based on a concept of whole plants having synergy as well as intelligence (Plant Intelligence). Examples of plant intelligence include key features that involve the ability to problem-solve in a flexible manner, anticipate the future, store memory, learn, communicate, and ultimately, be goal-oriented.1
I am thrilled to introduce you to The Mederi Center’s new healing room experience, which harnesses the combined therapeutic powers of vibroacoustic therapy, music, and specialized infrared light. If you don’t live near the Center in Ashland, Oregon, you may be able to seek out similar technologies offered at other healing centers.
Good Vibrations
The entire universe resonates with vibrations—some audible, others felt only through our bodies. This fundamental truth forms the foundation of our innovative approach to healing. Though it may seem ephemeral, the power of sound and vibration carries remarkable healing potential.
Beyond their aesthetic beauty, sound waves interact with our bodies at the cellular level, influencing our physical, mental, and emotional well-being. This understanding has led us to develop a comprehensive sound healing program that integrates advanced physics and biological principles to promote holistic health.
“The noblest foundation for medicine is love. It is love that teaches us the art of healing. Without love true healing can never be born.” – Paracelsus
Intravenous (IV) nutrient therapy, which most often includes vitamins, minerals, and sometimes botanical isolates has become very popular these days. IV vitamin C and cancer is a big topic in the world today. In very specific circumstances IV vitamin therapy can be excellent for people who have digestive disorders that prevent proper absorption of nutrients; however, don’t be fooled into thinking that this is an all-natural holistic medicine. It is extremely invasive, and at the massive pharmacological doses used, I don’t believe it’s good for you. We need to get back to gentle nourishing medicine that supports innate healing in a more unitive way.
Skin cancer is the most commonly diagnosed cancer in the US. Despite decades of widespread use of sunscreen and sunblock, the rates of the three main types of skin cancer—basal cell carcinoma, squamous cell carcinoma, and melanoma—are on the rise.[1]This concerning trend raises questions about the effectiveness of current sun protection methods and the factors contributing to skin cancer.
Fifty percent of all drugs, including cancer drugs marketed today, use the cytochrome P450 enzyme pathway for metabolism[1],[2] and frequently cause interactions. In brief, the cytochrome P4503A (CYP3A) subfamily is largely found in hepatocytes, with some presence in the intestine. Together with the transport protein P-glycoprotein (PGP) present in the small intestine, these 2 systems regulate metabolism of drugs and nutrients. Many foods, food components, and botanical supplements interact with the CYP3A and PGP metabolism, but even more importantly, an individual’s genome plays a significant role in how well one metabolizes and detoxifies various drugs including Aromatase and mTOR inhibitors. The effects of herbs on CYP3A and PGP is dose sensitive, meaning that often the dose would need to be very high in order to really impact these pathways. Another important factor is that much of the published research is either in vitro; animal in vivo, done with isolates (not whole herbs), and/or based on high dosages of these compounds. So, every referenced paper needs to be reviewed and analyzed for accuracy and relativity to how botanicals might impact both the effectiveness or toxicity of these and other drugs. The other factor is that to base interaction solely on P4503A and PGP is wrong. The ultimate question is still not answered, which is does this herbal combination either cause this drug to be less effective or does it increase the toxicity? In general, due to these nuances, evaluating the potential for negative drug-drug, nutrient-drug, or botanical-drug interactions metabolized through this pathway can be difficult and often lead to incorrect assumptions.
Many chemotherapeutic drugs have been used for the treatment of cancer, including doxorubicin, irinotecan, 5-fluorouracil, cisplatin, and paclitaxel. However, the effectiveness of chemotherapy is limited in cancer therapy due to drug resistance, therapeutic selectivity, and undesirable side effects.
Chemosensitization is one valuable strategy to overcome chemoresistance phenomena. Chemosensitization is based on the use of one drug to enhance the activity of another by influencing one or more mechanisms of resistance. The combination of therapies with natural compounds such as curcumin is likely to increase the effectiveness of drug treatment as well as reduce the incidence of adverse outcomes.
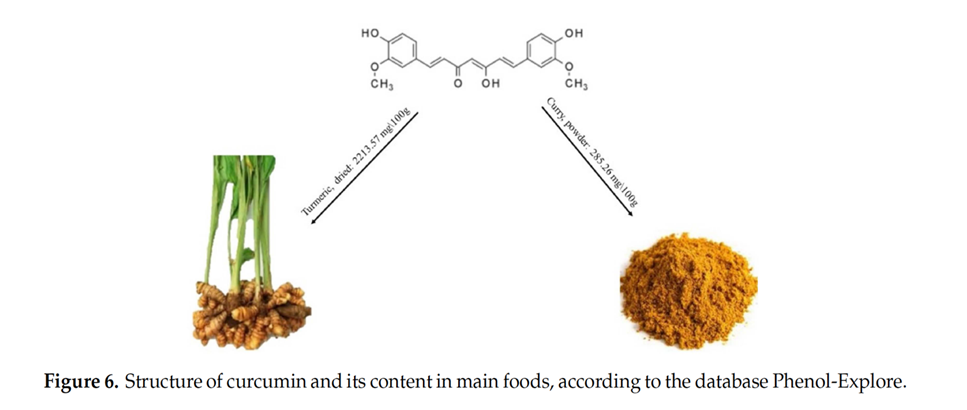
Curcumin, a polyphenolic isolated from Curcuma longa, belongs to the rhizome of Zingiberaceae plants.
Both in vitro and in vivo studies show that curcumin exerts many pharmacological activities with less toxic effects. Chemosensitization has been observed in cancers of the breast, colon, pancreas, gastric, liver, blood, lung, prostate, bladder, cervix, ovary, head and neck, and brain and in multiple myeloma, leukemia, and lymphoma. Similar studies have also shown that curcumin can sensitize a variety of tumors to gamma radiation including glioma, neuroblastoma, cervical carcinoma, epidermal carcinoma, prostate cancer, and colon cancer. The way in which curcumin acts as a chemosensitizer and radiosensitizer has been studied extensively. For example, it downregulates various growth regulatory pathways and specific genetic targets including genes for NF-κB, STAT3, COX2, Akt, antiapoptotic proteins, growth factor receptors, and multidrug-resistance proteins. Although it acts as a chemosensitizer and radiosensitizer for tumors in some cases, curcumin has also been shown to protect healthy organs such as the liver, kidney, oral mucosa, and heart from chemotherapy and radiotherapy-induced toxicity.[3]
The Bioavailability of Curcumin: Separating Truth from Fiction
Curcumin and other curcuminoids from Curcuma longa (turmeric) are important bioactive compounds exhibiting various pharmacological activities. Turmeric is widely consumed as part of the spice mix curry and as a dietary supplement. It has a long history of therapeutic application in traditional Asian medicine. The active components of turmeric, collectively known as curcuminoids, are among the most promising natural compounds studied across the globe today.
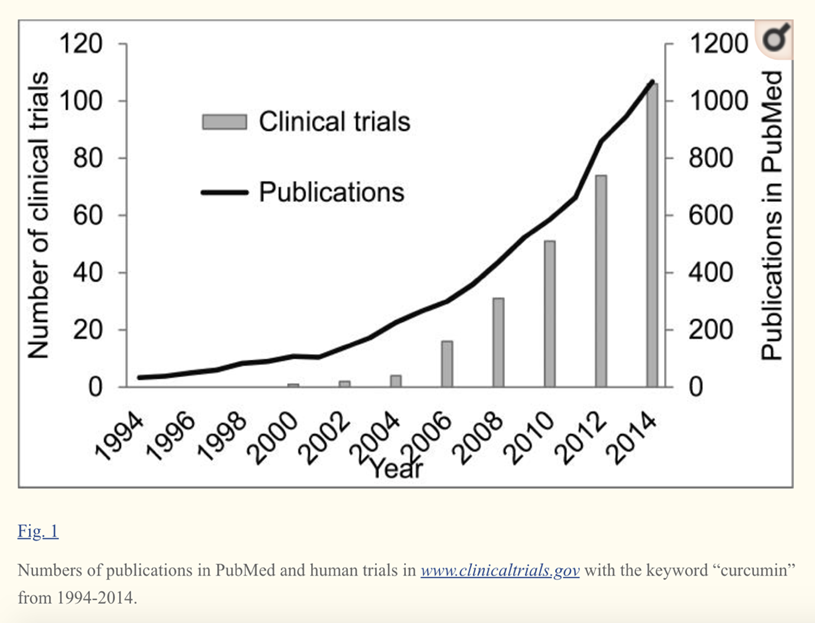
Clinical studies support the active role of curcuminoids in the management of chronic health conditions. Several pioneering studies have been conducted by major universities, research institutes and hospitals on Curcumin C3 Complex®, which have aided the understanding of the metabolic effects of curcumin.
Curcumin is a natural product with multiple biological activities and numerous potential therapeutic applications. However, the poor systemic bioavailability of the product fails to explain the potent pharmacological effects and hinders its clinical application.
The biological effects of curcumin in cellular and animal models are surprising considering its chemical and metabolic instability. Multiple studies have shown that, even with high doses of curcumin, the levels of curcumin in serum and tissues as well as its in vivo metabolites are extremely low after a short period of time.
With a lack of consensus on curcumin bioavailability and with various formulations making a variety of claims on the bioavailability (X times or XX times more than nearest competitor), consumers are understandably confused.
The reality is that after ingestion, little if any curcumin is present unchanged in systemic circulation.Furthermore, curcumin undergoes rapid non-enzymatic degradation in cell culture medium and possibly in vivo as well. Chemical transformation by human gut microbiota does not mean a loss in activity, but is actually a necessity for the therapeutic action of curcumin. Current thinking is that the molecular mechanisms of degradation of curcumin is necessary for interpreting in vitro and in vivo studies.
Compared to the parent compound curcumin, the degradation products mixture possessed higher O2.–-scavenging activity and stronger inhibition against fAβ formation. The docking simulations revealed that the bioactive degradation products make an important contribution to the experimentally observed enzymatic inhibition activities of curcumin.
Curcumin has been shown to possess low stability in aqueous solutions at physiological pH and degrades readily.. In phosphate buffer at pH 7.4, about 90% of curcumin degraded within 30 min and the degradation products have been identified as trans-6-(4′-hydroxy-3′-methoxyphenyl)-2,4-dioxo-5-hexenal, ferulic aldehyde, ferulic acid, feruloyl methane, vanillin, vanillic acid, and other dimerization end-products.
Selected degradation products mentioned above were the major human metabolites after curcumin consumption, and their levels were much higher than those of its metabolic compounds.
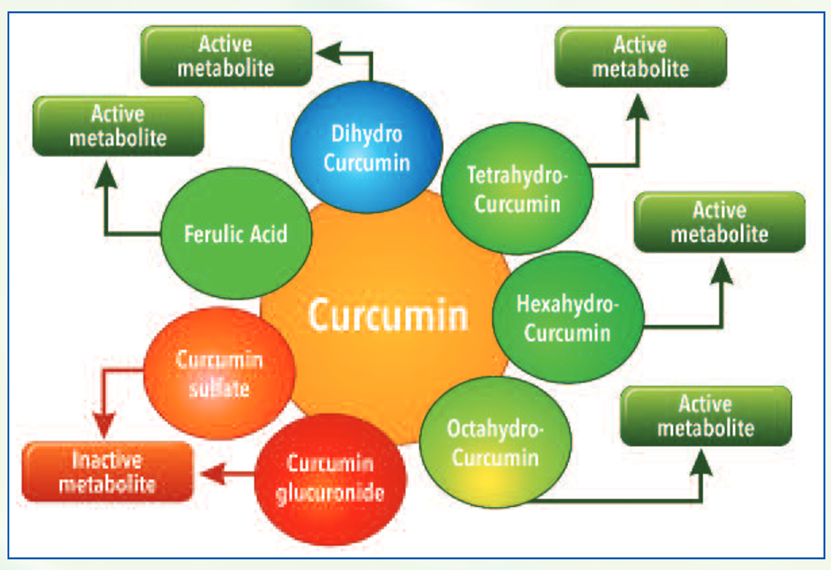
Upon ingestion, curcumin forms several active metabolites undergoing phase I metabolism such as dihydrocurcumin, tetrahydrocurcumin, hexahydrocurcumin and octahydrocurcumin.
In course of its metabolism, it also forms degradation compounds such as ferulic acid and bicyclopentadione. While these phase I metabolites have shown to have beneficial biological activity, compounds such as curcumin glucuronides and sulfates formed after phase II metabolism have shown to be ineffective in independent studies.
Given that curcumin is readily degraded under physiological condition, recent findings strongly suggested that the degradation products should make important contribution to the diverse biological activities of curcumin.[4],[5],[6],[7]
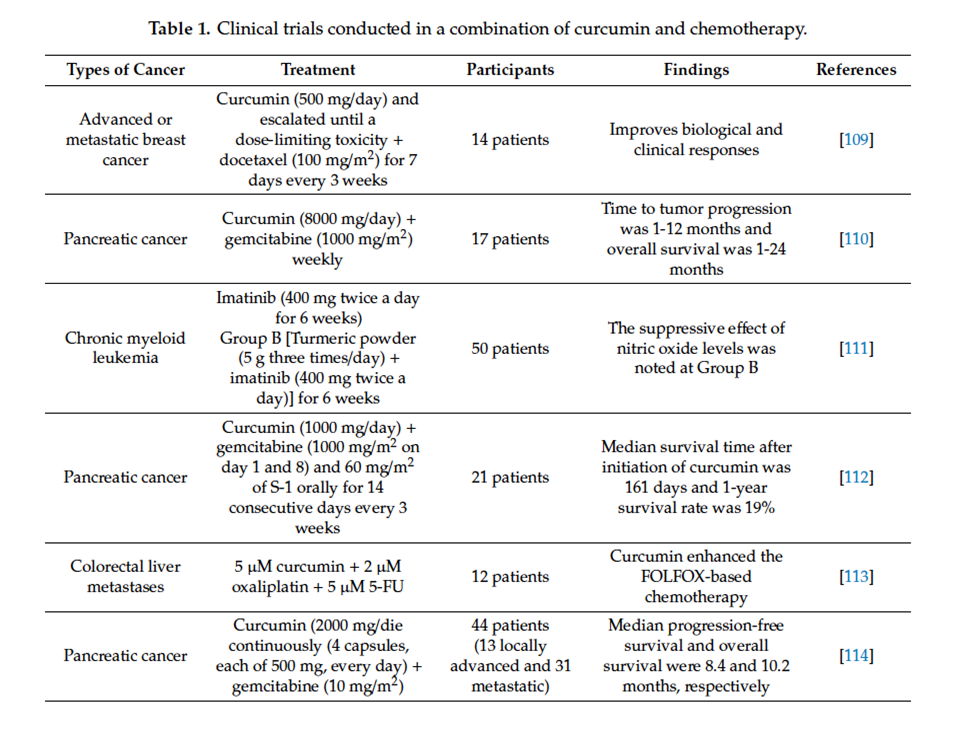
Oral curcumin also improved cachexia and general health in colorectal cancer patients.[8] In a phase II trial involving 21 patients with advanced pancreatic cancer, curcumin demonstrated bioactivity by downregulating nuclear factor-κB and cyclooxygenase-2. Despite limited absorption, antitumor response was seen in two patients.[9]
Curcumin Combined with Various Chemotherapeutic Agents
Combined with 5-FU
Research suggests that the combination of 5-FU and curcumin may overcome drug-resistance induced by 5-FU. Pre-treatment with curcumin (5 µM) enhanced the chemosensitization of 5-FU (0.1 µM) and reversed the multidrug resistance in resistant mismatch repair (MMR)-deficient human colon cancer cells compared to 5-FU alone.[10]
The combination of curcumin (10 μM) and 5-FU (0.1 mM)/oxaliplatin (5 μM) enhanced the synergistic antitumor activity in gastric cancer (BGC-823) cell lines compared to curcumin or 5-FU/oxaliplatin alone by downregulating the Bcl-2 mRNA and protein expression and activating the Bax and caspases-3, 8, and 9 expressions. This study further demonstrated that the combination of curcumin (10 mg/kg) and 5-FU (33 mg/kg)/oxaliplatin (10 mg/kg) shows potent growth inhibition of BGC-823 xenograft tumors compared to folinic acid, 5-FU, oxaliplatin (FOLFOX) or curcumin alone.[11]
A combination of curcumin (50 mg/kg/day for 40 days) and 5-FU (20 mg/kg once every 2 days for 40 days) inhibits cell proliferation against 5-FU resistant cells via suppression of epithelial-to-mesenchymal transition (EMT) compared to 5FU alone.[12]
In the context of breast cancer, a combination of curcumin (10 µM) and 5-FU (10 µM) significantly inhibited cell viability and enhanced apoptosis compared to 5-FU alone in vitro.[13]
In addition to the effects mentioned above, research indicates that combining 5-FU (50 µmol/L) and curcumin (25 µmol/L) can enhance the cytotoxicity against human gastric cancer (AGS) cells compared to 5-FU or curcumin alone.
In a further study focused on inflammation outcomes, this study found that the protein expression of COX-2 and NF-κB in human gastric cancer (MKN45) cells were diminished after co-treatment with 5-FU (50 µmol/L) and curcumin (25 µmol/L). This finding implies that curcumin sensitizes gastric cancer cells to 5-FU by modulating inflammatory molecules. The anti-gastric cancer activity is shown not only in in vitro study, but data from an animal study further demonstrated that curcumin enhanced the anticancer activity of 5-FU (52 mg/kg 5-FU + curcumin 74 mg/kg, every 3 days for 6 times in total) compared to 5-FU or curcumin alone, and without increasing the toxicity in nude mice bearing MKN45 tumor xenografts.[14]
Combined with Doxorubicin
Doxorubicin, one of the active single-agent drugs, is widely used for the treatment of cancers, including leukemia, lung, brain, prostate, ovarian, and breast. However, the clinical use of doxorubicin often led to critical cardiotoxicity and developed multidrug resistance. Substantial evidence showed that curcumin (4 mg/kg every 2 days for a total of 7 injections) exhibits a better treatment efficacy of doxorubicin (0.4 mg/kg) in cancer due to the efflux inhibitory effect of curcumin.[15],[16],[17],[18]
A study conducted by Guorgui et al.[19] has shown that combination of curcumin (5 µM) and doxorubicin (0.4 mg/mL) demonstrated a stronger additive effect by reducing the proliferation of Hodgkin lymphoma (L-540) cells by 79%. The pharmacokinetic study also revealed that curcumin (5 mg/kg) could enhance the absorption of doxorubicin (5 mg/kg) and decrease drug efflux in vivo, suggesting that curcumin downregulates the intracellular levels of ATP-binding cassette (ABC) drug transporters.[20]
While DOX alone does not decrease tumor weight, the combination of DOX and curcumin has been shown to significantly reduce tumor weight to 56.5% (p<0.05) to that of the control group. In combination, curcumin enhanced apoptosis by DOX and decreased cell viability. The curcumin-DOX combination also suppressed activation of caspase-3, -8, and -9 compared to DOX alone. It appears that curcumin increases DOX-induced antitumor activity by suppressing the main caspase pathway and activating the main caspase independent pathway. The combination of curcumin and DOX suppressed the reduction of glutathione peroxidase activity and increased lipid peroxide levels in the heart. Therefore, it is expected that curcumin may reduce the adverse reactions associated with DOX. According to researchers, results suggest that curcumin can be used as a modulator to enhance the therapeutic index of cancer patients and improve their QOL.[21]
Combined with Platin Agents
Cisplatin-based combination therapy has emerged as a standard therapy for metastatic and advanced bladder cancer,[22] demonstrating 15–20% improved survival and 50–70% response rate. However, nearly 30% of patients do not respond to initial chemotherapy and show recurrence within 1 year.[23] Cisplatin is an inorganic platinum agent which can induce DNA-protein and interstrand and intrastrand DNA crosslinks.[24]
While this crosslink can induce apoptosis and inhibit cell proliferation,[25] the efficacy of cisplatin is limited by the development of cell resistance. Co-treatment with curcumin (10 µM) and cisplatin (10 µM) has shown a potent synergistic effect by activating caspase-3 and upregulating phospho-mitogen-activated protein kinase (p-MEK) and phospho-extracellular signal-regulated kinase 1/2 (p-ERK1/2) signaling in bladder cancer cell lines (253J-Bv and T24) compared to curcumin or cisplatin alone.[26] In addition to the effects observed on bladder cancer, the combination of curcumin and cisplatin was shown to upregulate the expression of miR-186 via modulation of Twist1 in ovarian cancer compared to cisplatin alone.[27]
Synergism of Curcumin and Epigallocatechin-3-gallate
Drug resistance remains an ongoing challenge in ovarian cancer chemotherapy. Research has investigated the synergism in activity from the sequenced combinations of cisplatin (Cis) with curcumin (Cur) and epigallocatechin-3-gallate (EGCG) in ovarian cancer cell lines. The drugs were added in binary combinations: Cis combined with Cur, and Cis combined with EGCG to the human ovarian A2780 and A2780(cisR) cancer cell lines, using five different sequences of administration: 0/0 h, 4/0 h, 0/4 h, 24/0 h and 0/24 h. Addition of Cis 4 h before Cur and EGCG (0/4 h combination) produced the most synergistic outcomes in both the A2780 and A2780(cisR) cell lines. The cellular accumulations of platinum and platinum-DNA binding resulting from the 0/4 h combinations were greater as compared to the values using Cis alone, thus providing an explanation for the synergistic action. When sequenced combinations of Cis with Cur and with EGCG are applied to human ovarian A2780 and A2780(cisR) cancer cell lines, lower concentrations and shorter time gap between the two additions seem to produce a higher cytotoxic effect.[28]
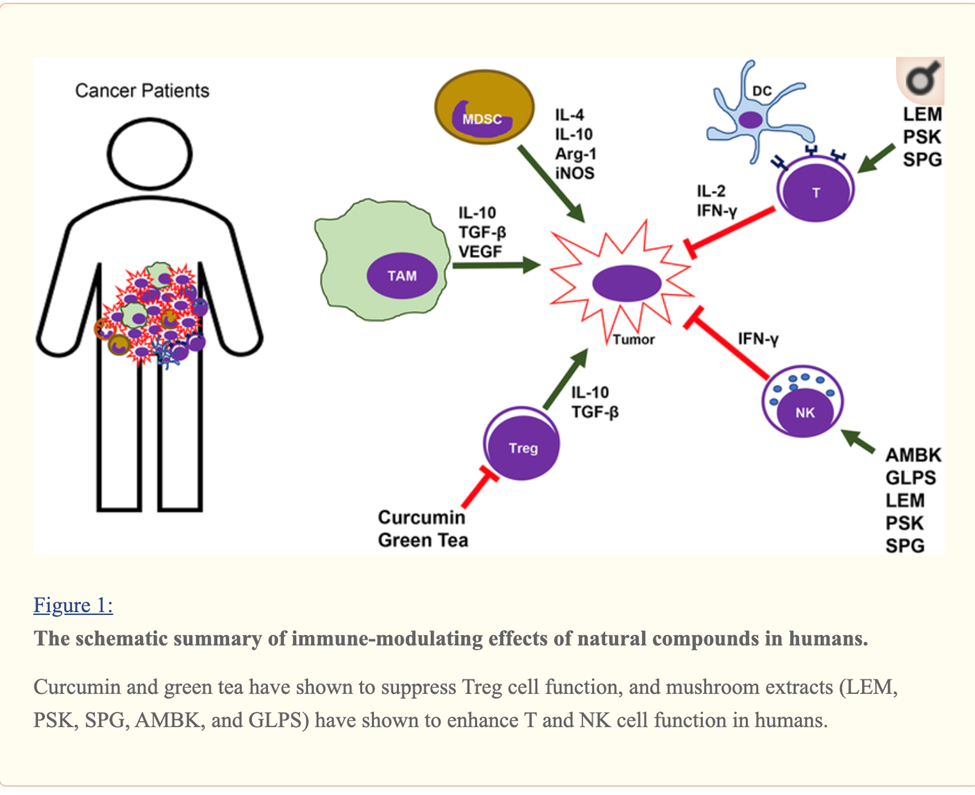
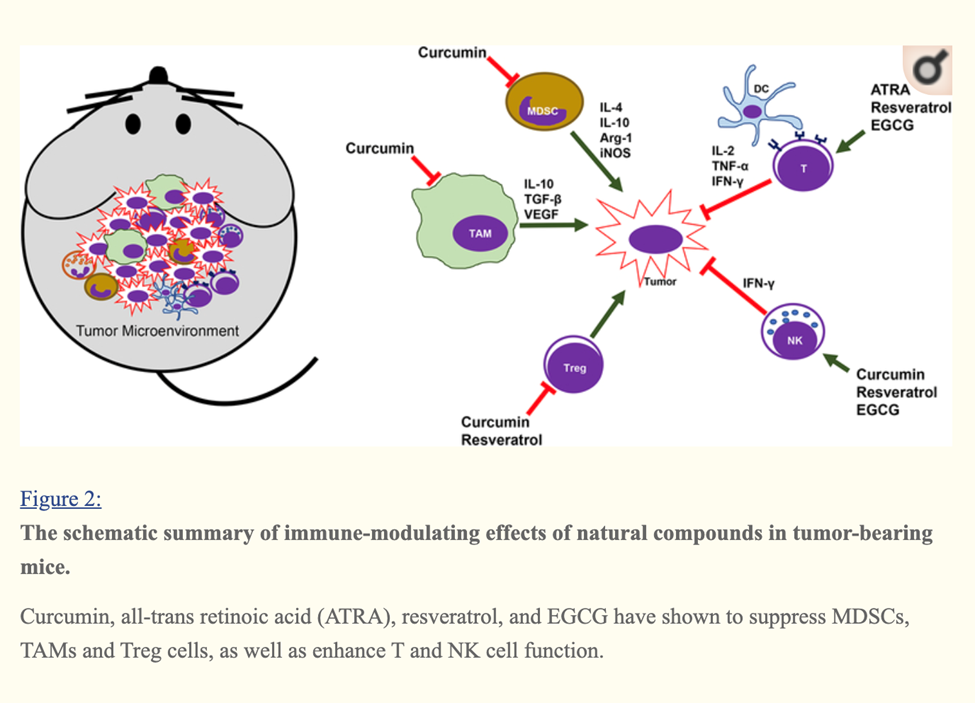
Curcumin, EGCG (Green tea extract) and Resveratrol Immune Enhancing Anti-tumor
Curcumin, Resveratrol, EGCG and Beta glucan rich mushroom extract have shown promising immune-modulating effects, such as inhibiting myeloid-derived suppressor cells and enhancing natural killer and cytolytic T cells, in tumor-bearing animal models.
Many other studies involving either genetic models or xenograft models of other types of cancer have demonstrated that curcumin can reverse the tumor-favoring microenvironment, leading to further investigations of curcumin combined with standard cancer therapies. One study combined the anti-PD-L1 antibodies with bisdemethoxycurcumin (BDMC), a natural dimethoxy derivative of curcumin, in C57BL/6 mice with metastasized bladder cancer (MB49 cells).
They observed that BDMC alone increased levels of tumor-infiltrating CD8+ T cells, IFN-γ secretion in the blood, and decreased the number of tumor-infiltrating MDSCs.
Importantly, the combination of anti-PD-L1 antibodies with curcumin further enhanced the secretion of IFN-γ, granzyme B, and perforin from CD8+ T cells.[29]
Furthermore, curcumin has been combined with vaccines against tumor development. For instance, one group applied two vaccination strategies to BALB/c mice bearing triple-negative breast tumors (4T1 cells). One strategy gave the mice curcumin and all the vaccinations after tumors had developed. The other treated the mice with curcumin before they were inoculated with tumor cells and then vaccinated the animals after tumors developed. Interestingly, the second strategy was more effective against metastasis than the first, as it decreased the production of pro-inflammatory cancer promoting cytokines (IL-6), and increased levels of anti-tumor cytokines (IL-12 and IFN-γ).[30]
A cocktail of Turmeric- curcumin, Green tea epicatechin gallate and resveratrol—increased levels of tumor-infiltrating NK cells and CD8+ cytolytic T cells in C57BL/6 mice bearing HPV+ mouse lung cancer (TC-1 cells).
The combination formula repolarized tumor promoting M2-like TAMs to tumor fighting M1-like TAMs in the tumors.[31]
Combined with Taxanes
Docetaxel (30 or 75 mg) has been clinically approved and widely used for the treatment of metastatic castration-resistant prostate cancer.[32] However, prolonged treatment with docetaxel can cause severe toxicity in patients. A study found that the combined treatment of docetaxel (10 nM) and curcumin (20 µM) for 48 h significantly inhibited proliferation and induced apoptosis in prostate cancer (PC-3) (DU145 and PC3) cells compared to curcumin and docetaxel alone. The data further demonstrated that curcumin enhances the efficacy of docetaxel in PC-3 cells via modulation of COX-2, p53, NF-κB, phospho-Akt, PI3K, and receptor tyrosine kinase (RTK).[33] This finding implies that combining curcumin with conventional chemotherapy may act as an effective treatment regimen for patients with prostate cancer to reduce cytotoxicity and overcome drug-resistance induced by docetaxel.
Curcumin is a taxane sensitizer for tumors and chemoprotector for normal organs, including in cases of lung cancer.[34]
Curcumin induces apoptosis and inhibits the growth of orthotopic human non-small cell lung cancer xenografts. A research study evaluated the effect of curcumin on the expression of nuclear factor κB-related proteins in vitro and in vivo and on growth and metastasis in an intralung tumor mouse model.
H1975 NSCLC cells were treated with curcumin (0-50μM) alone, or combined with gemcitabine or cisplatin. The effects of curcumin were evaluated in cell cultures and in vivo, using ectopic and orthotopic lung tumor mouse models. Western blot analysis showed that the expressions of IkB, nuclear p65, cyclooxygenase 2 (COX-2) and p-ERK1/2 were down-regulated by curcumin in vitro. Curcumin potentiated the gemcitabine- or cisplatin-mediated antitumor effects. Curcumin reduced COX-2 expression in subcutaneous tumors in vivo and caused a 36% decrease in weight of intralung tumors (P=.048) accompanied by a significant survival rate increase (hazard ratio=2.728, P=.036). Curcumin inhibition of COX-2, p65 expression and ERK1/2 activity in NSCLC cells was associated with decreased survival and increased induction of apoptosis. Curcumin significantly reduced tumor growth of orthotopic human NSCLC xenografts and increased survival of treated athymic mice. Researchers note that to evaluate the role of curcumin in chemoprevention and treatment of NSCLC, further clinical trials are required.[36]
Curcumin Induces PTEN and Improves the Cytotoxicty of Gemzar Against Pancreatic Cancer
Curcumin induces cancer cell growth arrest and apoptosis in vitro, but its poor bioavailability in vivo limits its antitumor efficacy. Researchers noted that in previous evaluations of the bioavailability of novel analogues of curcumin compared with curcumin, they found that the analogue CDF exhibited greater systemic and pancreatic tissue bioavailability.
In a study reported in Cancer Research, scientists evaluated the effects of CDF or curcumin alone or in combination with gemcitabine on cell viability and apoptosis in gemcitabine-sensitive and gemcitabine-resistant pancreatic cancer (PC) cell lines. Mechanistic investigations revealed a significant reduction in cell viability in CDF-treated cells compared with curcumin-treated cells, which were also associated with the induction of apoptosis, and these results were consistent with the downregulation of Akt, cyclooxygenase-2, prostaglandin E(2), vascular endothelial growth factor, and NF-kappaB DNA binding activity.
The researchers documented attenuated expression of miR-200 and increased expression of miR-21 (a signature of tumor aggressiveness) in gemcitabine-resistant cells relative to gemcitabine-sensitive cells. Interestingly, CDF treatment upregulated miR-200 expression and downregulated the expression of miR-21, and the downregulation of miR-21 resulted in the induction of PTEN. These results prompt further interest in CDF as a drug modality to improve treatment outcome of patients diagnosed with PC as a result of its greater bioavailability in pancreatic tissue.[37]
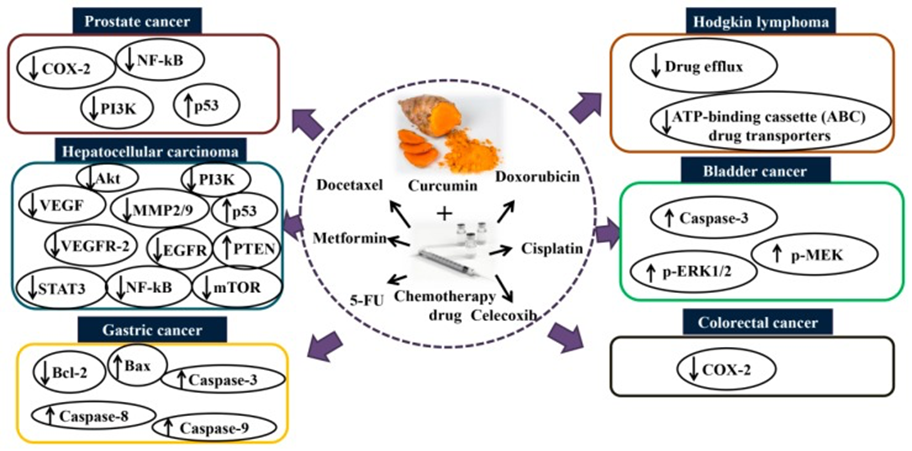
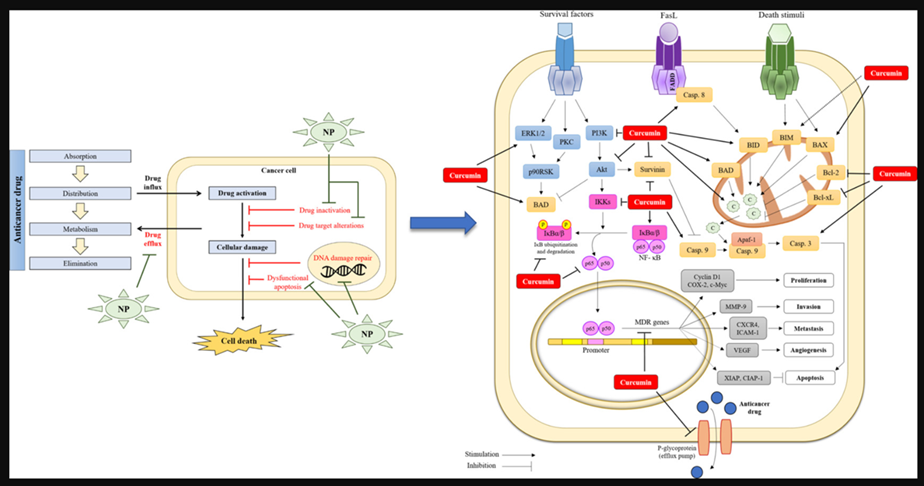
Mechanisms of action of combination curcumin and chemotherapy drugs in vitro and in vivo. Co-treatment with curcumin and chemotherapy drugs such as docetaxel, metformin, 5-fluorouracil, doxorubicin, cisplatin, and celecoxib enhance the synergistic effect via modulating several signaling pathways and thus inhibit cancers such as prostate, hepatocellular, gastric, Hodgkin lymphoma, bladder, and colorectal. Akt: protein kinase B; COX-2: cyclooxygenase-2; EGFR: epidermal growth factor receptor; MMP2/9: matrix metalloproteinase-2/9; mTOR: mammalian target of rapamycin; NF-κB: nuclear factor kappa B; p-ERK1/2: phospho-extracellular signal-regulated kinase 1/2; PI3K: phosphoinositide 3-kinase; p-MEK: phospho-mitogen-activated protein kinase; STAT3: signal transducer and activator of transcription 3; VEGF: vascular endothelial growth factor; VEGFR2: vascular endothelial growth factor receptor 2.
Paclitaxel (PTX) is a key member of the taxane family with potential anti-tumor activity against different cancers. Notably, PTX has demonstrated excellent proficiency in elimination of cancer in clinical trials. This chemotherapeutic agent is isolated from Taxus brevifolia and is a tricyclic diterpenoid. However, resistance of cancer cells into PTX chemotherapy has endangered its efficacy. In addition, administration of PTX is associated with a number of side effects such as neurotoxicity, hepatotoxicity, and cardiotoxicity, demanding novel strategies in obviating PTX issues.
Curcumin is a pharmacological compound with diverse therapeutic effects including anti-tumor, antioxidant, anti-inflammatory, and anti-diabetic properties. Curcumin appears to enhance the anti-tumor activity of PTX against different cancers. Additionally, curcumin administration reduces the adverse effects of PTX due to its excellent pharmacological activities.[40]
Combined with Metformin
Data from an in vitro study showed that combining metformin (10 mM) and curcumin (5 and 10 µM) can induce apoptosis and inhibit metastasis and invasion in HepG2 and PLC/PRF/5 cells. The anticancer effects could be attributed to the vascular endothelial growth factor (VEGF), MMP2/9, and vascular endothelial growth factor receptor 2 (VEGFR-2) inhibition, PTEN and p53 activation, and epidermal growth factor receptor (EGFR)/STAT3 and NF-κB/mTOR/Akt/PI3K suppression. Data from an in vivo study further showed that co-treatment with metformin and curcumin significantly suppressed hepatocellular carcinoma compared to curcumin (60 mg/kg) and metformin (150 mg/kg) alone in a xenograft mouse model.[41]
Combined with Celecoxib and COX-2 inhibitor
Celecoxib is another selective inhibitor of COX-2, an enzyme induced by different stimuli including inflammation.[42] Celecoxib (75 µM for 16 h) has shown an ability to induce apoptosis and suppress tumor angiogenesis in several types of cancer.[43] However, the long-term use of Celecoxib leads to an adverse outcome such as cardiovascular toxicity.[44] The combination of curcumin and Celecoxib was shown to reduce cancer cell growth in vitro compared to Celecoxib alone. A study reported by Lev-Ari et al. revealed that curcumin (10–15 µmol/L) and physiological dosage of Celecoxib (5 µmol/L) exhibited a synergistic inhibitory effect against human colorectal cancer (HT-29) cells. The study showed that the combination of curcumin and Celecoxib induces apoptosis in HT-29 cells via downregulation of COX-2 expression, suggesting that curcumin synergistically augments the growth inhibitory effects of Celecoxib in human colon cancer cell lines in vitro.[45]
Another anti-cancer property of curcumin seems to be overcoming multidrug resistance.[46] For example, it inhibits P-glycoprotein expression in mouse leukemia L1210/Adr cell lines. Cells treated with a combination of PI3K inhibitor and curcumin displayed lower P-glycoprotein expression in comparison to cells treated only with PI3K inhibitor. It was suggested that curcumin may act by inhibition of the PI3K/Akt/ NF-κB pathway.[47]
Curcumin was found to be a safe and non-toxic dietary supplement. Its efficacy of was studied during clinical trials.[48],[49]
In the mouse model, a high curcumin supplementation (100 mg/kg) was able to improve glucose and insulin intolerance through activating the AMPK pathway, showing the potential involvement of curcumin in metabolism.[50] Modulation of AMPK (AMP-activated protein kinase) improves glucose/insulin efficiency and adds the cancer suppressing effects of curcumin. AMPK acts as a cellular energy sensor, and curcumin selectively can enhance normal cell AMPK signaling, while suppressing it within the cancer cell. [51],[52]
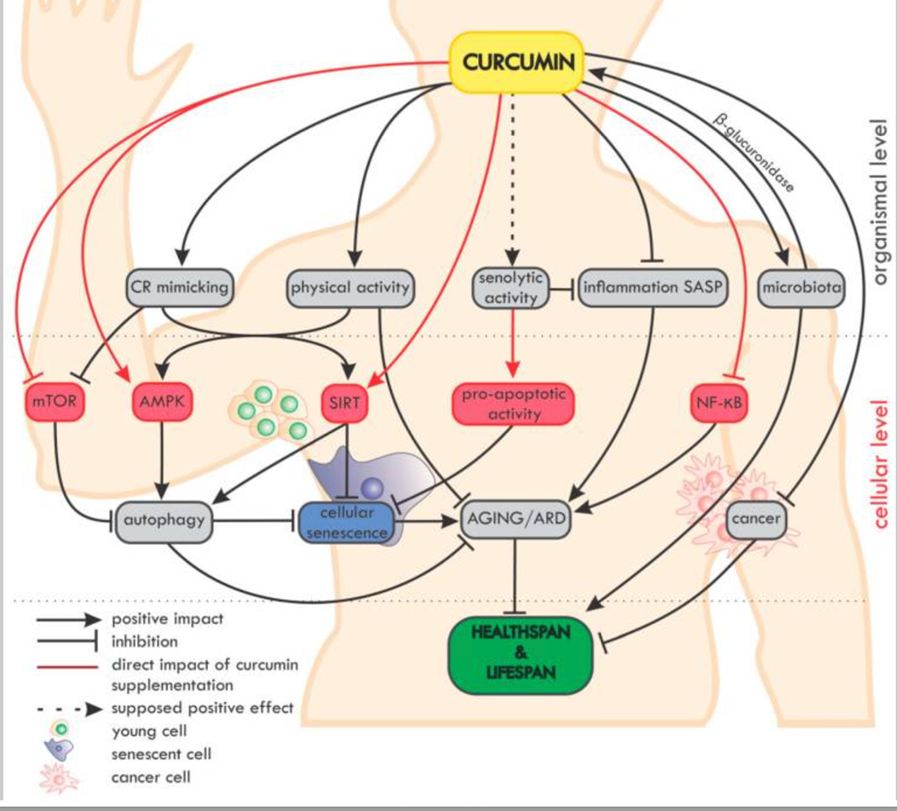
Curcumin in the Modulation of Aging
Overview of the impact of curcumin on ageing and age-related diseases (ARD) at the organismal and cellular level. On the organismal level, curcumin mimics caloric restriction (CR) and improves the effectiveness of physical activity (which mimics CR).[53]
In Conclusion
Natural compounds, including curcumin, resveratrol, EGCG, and β-glucan have shown synergistic promising immune-modulating, anti-tumor, and chemo-potentiating effects.
The results of these clinical studies are conclusive, and these studies have established a good foundation for further research focusing on implementing curcumin along with other botanical compounds in clinical oncology. It’s important to note, however, that I never use it as a soloist! I always use a formula that combines curcumin with EGCG, resveratrol, grape seed extract, quercetin, and other botanical extracts. This provides a harmonious approach that best supports healing.
[2] Zhou SF, Xue CC, Yu XQ, Li C, Wang G. Clinically important drug interactions potentially involving mechanism-based inhibition of cytochrome P450 3A4 and the role of therapeutic drug monitoring. Ther Drug Monit. 2007 Dec;29(6):687-710. doi: 10.1097/FTD.0b013e31815c16f5. PMID: 18043468.
[3] Goel A, Aggarwal BB. Curcumin, the golden spice from Indian saffron, is a chemosensitizer and radiosensitizer for tumors and chemoprotector and radioprotector for normal organs. Nutr Cancer. 2010;62(7):919-30. doi: 10.1080/01635581.2010.509835. PMID: 20924967.
[4] Majeed M. The Age of Biotransformation, 2015; Personal communication. Ganjali S, Sahebkar A, Mahdipour E, Jamialahmadi K, Torabi S, Akhlaghi S, Ferns G, Parizadeh SM, Ghayour-Mobarhan M. The Scientific World Journal 2014; doi 10.1155/2014/898361
[5]Liang Shen, Cui-Cui Liu, Chun-Yan An, Hong-Fang Ji, How does curcumin work with poor bioavailability? Clues from experimental and theoretical studies, Scientific Reportsvolume 6, Article number: 20872 (2016), Published: 18 February 2016