
Omicron and the Vaccine Conundrum
With record levels of Covid cases at an all-time high since the onset of the pandemic due to the latest highly transmissible Omicron variant[1] ,people across the globe are increasingly fed up with ineffective methods to control the transmission by lockdowns, mandates and inoculating the planet. As we head into the third year of the virus, it’s time for governing bodies to change the strategy for living in a post-pandemic world.
Recently, a leading Israeli Immunologist, Professor Ehud Qimron, head of the Department of Microbiology and Immunology at Tel Aviv University declared, in an open letter to the Israel Health Ministry regarding COVID-19 policy [2]: “The truth is that you have burned hundreds of billions of shekels to no avail – for publishing intimidation, for ineffective tests, for destructive lockdowns, and for disrupting the routine of life in the last two years.” He goes on to say: “In the end, the truth will always be revealed, and the truth about the coronavirus policy is beginning to be revealed. When the destructive concepts collapse one by one, there is nothing left but to tell the experts who led the management of the pandemic – we told you so.”
In the widely circulated letter, he goes on to say:
- “Over the past 2 years we had heard over and over again, you defeated it, but you haven’t.
- You refused to admit that mass testing is ineffective.
- You refused to admit that recovery is more protective than a vaccine, despite previous knowledge and observations showing that non-recovered vaccinated people are more likely to be infected than recovered people (meanwhile, a new CDC Study[3] just confirmed that natural immunity provides significantly more protection against COVID than vaccination).
- You refused to admit that the vaccinated are contagious despite the observations. Based on this, you hoped to achieve herd immunity by vaccination – and you failed in that as well.
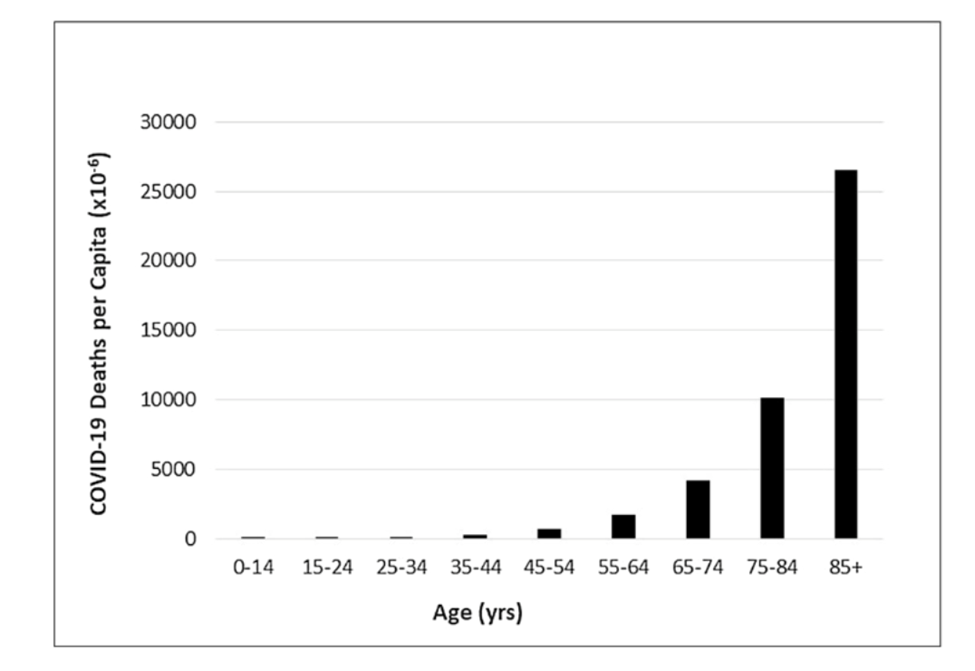
- You insisted on ignoring the fact that the disease is dozens of times more dangerous for risk groups and older adults than for young people who are not in risk groups, despite the knowledge that came from China as early as 2020.
His letter also criticizes the fact that they have ignored, and even worse, ridiculed, slandered, distorted, and discredited, the expressed “grave” concerns by an extraordinarily large group of infectious disease epidemiologists, public health scientists, and medical professionals about the damaging physical and mental health impacts of the prevailing COVID-19 policies.
Meanwhile, despite the mass censorship in the US that has silenced the voices of anyone opposing the mainstream narrative, many are independently seeking out and following the science published in reputable, peer-reviewed journals by physicians, immunologists, molecular biologists, epidemiologists, and virologists, and are bringing credible facts, studies, and legitimate concerns into public view.
I believe any reasonable-thinking person will soon come to the conclusion that the vaccines are not the only answer to ending the pandemic. Even Bill Gates, in a discussion last week regarding the vaccine’s effectiveness, discussed the fact that they don’t prevent transmission and the duration of protection is limited (in fact, they are rapidly ineffective against Delta and even more-so against Omicron). In early December of last year, Moderna President, Stephen Hoge also admitted to the “dent in the vaccine’s efficacy”, especially against Omicron.
In the latest issue of the journal Nature, immunologists Wendy Burgers and Catherine Riou, who both work at the University of Cape Town in South Africa, had studied previous variants and found that, although the emerging coronaviruses weakened people’s antibody defenses, another arm of the immune system — mediated by specialized cells called T cells — could still recognize the pathogens.[4]
The Omicron variant, as well as potentially future variants, remain highly susceptible to T-cell responses.[5],[6],[7] So, natural immunity, from previous COVID-19 infection, may offer more protection against Omicron, because of the more robust immune response that occurs, compared to vaccine immunity; but that doesn’t rule out some protection with vaccines, especially in those that developed T-cell immunity, as opposed to antibody immunity.
Studies have analyzed T-cells taken from people who have either received a COVID-19 vaccine or been infected with a previous variant, and found that these T-cells can respond to Omicron. These cells perform a variety of immune functions, including acting as ‘killer’ cells that destroy virus-infected cells. By killing infected cells, T-cells can limit the spread of infection — and potentially reduce the chance of serious illness.
How Does Omicron Outsmart our Current Vaccines?
An extremely reliable artificial intelligence (AI) model called TopNetmAb has been used by molecular biologists and mathematicians in the US since the beginning of the pandemic to successfully predict the mutations of the SARS-CoV-2 with high chances of becoming significantly more infectious and those most likely to escape the vaccines. In fact, this work has been sponsored by Bristol-Myers Squibb, Pfizer, and NIH and is available on the Pub-Med database. In early 2020, they provided a list of more than 15 “most likely vaccine escape receptor binding domain (RBD) mutations” predicted by the model, “all of which are detected in the variants of concern and variants of interest denounced by the World Health Organization”, including Delta and Omicron. In April of 2021, they “provided a list of 31 RDB mutations that may weaken most of the binding to antibodies”. The purpose of their latest research, published in early December 2021, was to analyze how the RDB mutations on the Omicron variant would affect infectivity and efficacy of existing vaccines and antibody drugs. They concluded that Omicron’s ability to escape the vaccines is about twice as high as that of the Delta variant and that the currently available monoclonal antibodies are extremely compromised, with the exception of Regeneron.
According to the researchers reporting on the infectivity, vaccine breakthrough, and antibody resistance of COVID-19, the Omicron variant carries an unusually high number of mutations on the spike (S) protein, the main antigenic target of antibodies generated by either infections or vaccination. The authors note that any mutation on the S protein receptor binding domain would cause immediate concerns about the efficacy of existing vaccines, monoclonal antibodies and the potential of reinfection. They also state that Omicron may be induced by vaccination. In other words, the vaccines we are using are potentially what’s causing the mutations to occur, much like what happens from antibiotic abuse and antibiotic resistance. In comparison, the devastating Delta variant has only 5 S protein mutations, which initially posed a high potential global risk and has since spread internationally.
“The mutations on the Omicron variant are widely distributed on multiple proteins of SARS-CoV-2 such as NSP3, NSP4, NSP5, NSP6, NSP12, NSP14, S protein, envelope protein, membrane protein, and nucleocapsid protein. The focus is the mutations on the S protein receptor-binding domain (RBD) for the potential impact on infectivity and antibody resistance caused by this new variant. This is due to the fact that the RBD located on the S protein facilitates the binding between the S protein and the host angiotensin-converting enzyme 2 (ACE2). Such S-ACE2 binding helps the SARS-CoV-2 enter the host cell and initiates the viral infection process.”[8]
The TopNetmA AI model, which has been extensively validated over the past 1.9 years, was used to predict the binding free energy (BFE) changes induced by specific Omicron mutations at the S protein-ACE2/antibody complex.
“Omicron may be over ten times more contagious than the original SARS-CoV-2 and about twice as infectious as the Delta variant, mainly due to its RBD mutations N440K, T478K, and N501Y. Additionally, Omicron has a high potential to disrupt the binding of most 132 antibodies with the S protein, mainly due to its RBD mutations K417N, E484A, and Y505H, indicating its stronger vaccine breakthrough capability than the Delta variant.” The authors also identified mutations that would seriously reduce the efficacy of the monoclonal antibodies (mAb) however, Omicron’s impact on the Regeneron mAb cocktail is predicted to be mild.
What Justification is there for Vaccine Mandates, Especially in Children and Low-Risk Populations?
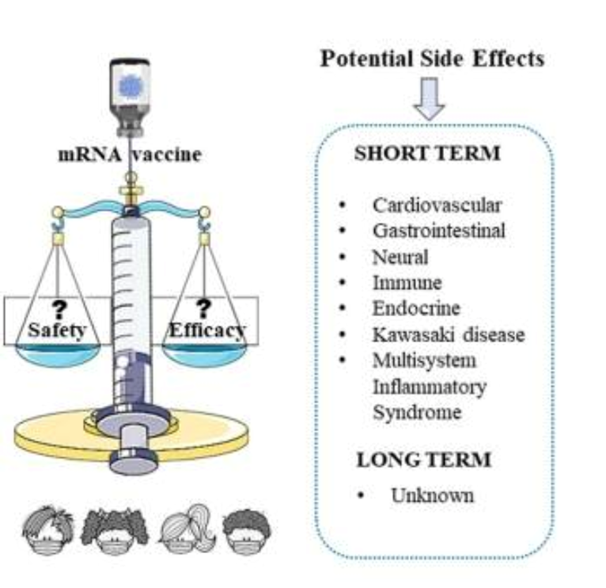
As experts have well stated, Omicron is a gamechanger! With a variant that causes symptoms similar to the common cold and flu, does not cause severe respiratory illness requiring oxygen and ventilators, and an extremely low risk of death, there really is no reason for vaccine mandates; especially ones that leak, have little to no benefit anymore, and require frequent boosters that quickly wane in effectiveness. It is also becoming increasingly recognized, according to in-hospital data and the Vaccine Adverse Event Reporting System (VAERS), that there are numerous potential risks from the vaccines for which we have no long-term data as well as limited and possibly flawed studies regarding the safety of this new gene transfer technology.
The strongest argument for COVID-19 vaccine mandates has been that it’s not only about protecting one-self, but reducing the chances of spreading infection to others, and thereby participating in the global battle against the virus. Unfortunately, with these vaccines, we cannot expect the same result as the protein-based vaccines of old, used to eliminate highly contagious and deadly diseases such as measles and small-pox, which, contrary to COVID-19, spread rapidly among children with devastating effects and the vaccines can indeed be credited for saving lives. We now know there is no compelling evidence that the vaccines are generally effective at slowing the spread of Omicron. Vulnerable populations such as those over the age of sixty-five, especially the elderly, and those with pre-existing conditions, should carefully weigh the risk to benefit while the rest of society, especially children, should no longer live in fear and focus on non-pharmaceutical interventions and lifestyle practices to live a healthy, Covid-free life.
New evidence is strong that vaccinations do not reduce transmission by those who have been vaccinated. A study published in October, 2021, in the European Journal of Epidemiology, a monthly peer-reviewed medical journal, examined 168 countries and 2,947 counties in the United States and concluded that higher vaccination rates are not associated with fewer COVID cases.[9] Many people believe that vaccine mandates need to be stopped, especially for our children where they pose potentially more harm than good; besides they are enormously costly.[10]
The World Health Organization’s (WHO) chief scientist Soumya Swaminathan said Tuesday that there is no current evidence that suggests healthy adolescents or children need COVID-19 vaccine booster doses. Speaking at a news briefing, Swaminathan explained that more research is necessary on the shots going forward, and that the agency had been making decisions based on current science. “There is no evidence right now that healthy children or healthy adolescents need boosters. No evidence at all,” she said. Swaminathan said a panel would meet later this week to consider the question of how countries should be giving out boosters “with the view to reducing deaths.”
According to a toxicology report published in the journal Elsevier in July of 2021 titled “Why are we vaccinating children against COVID-19”: “Clinical trials for these inoculations were very short-term (a few months), had samples not representative of the total population, and for adolescents/children, had poor predictive power because of their small size. Further, the clinical trials did not address changes in biomarkers that could serve as early warning indicators of elevated predisposition to serious diseases. Most importantly, the clinical trials did not address long-term effects that, if serious, would be borne by children/adolescents for potentially decades.”
COVID-19, SARS-CoV-2, Inoculation, mRNA vaccines, Viral vector vaccines, Adverse events, Vaccine Safety
Last month, Pfizer and BioNTech announced that their COVID-19 vaccine failed to rouse a sufficient antibody response in children between two and five years old. As a result, the vaccine hasn’t been authorized in the United States for children under five.[12]
COVID-19 and Vaccine Related Heart Conditions in Youth
The incidence of myocarditis increased after the receipt of the BNT162b2 Pfizer COVID-19 vaccine, particularly after the second dose among young male recipients; with the largest difference among male recipients between the ages of 16 and 19 years.[13]
Myocarditis (myo=muscle, card=heart, itis=inflammation) is a condition in which the heart muscle cells become inflamed and don’t function properly.
According to a study published on December 18, 2021, from the University of Oxford, people under the age of 40 were shown to have a higher risk of heart disease when they received the Moderna mRNA vaccine than when they contracted COVID-19. As a result, people who received two doses of Moderna’s COVID-19 vaccine had a rate of 15 or more myocarditis cases per million people. The risk of myocarditis doubles with each vaccine dose in men under 40 – and is sharply higher than the risk from the coronavirus infection itself. [14]
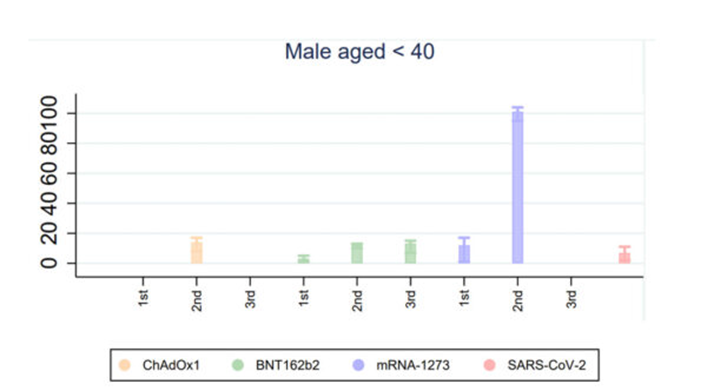
Vaccinations with Moderna’s mRNA-1273 was associated with a significantly increased risk of myocarditis or myopericarditis in the Danish population, primarily driven by an increased risk among individuals aged 12-39 years, while BioNTech and Pfizer’s Comirnaty BNT162b2 vaccination was only associated with a significantly increased risk among women.[15]
And finally, a systematic review, that included sixty-nine studies, including 43 case reports and 26 case series, were included. Myocarditis/myopericarditis and pericarditis were the most common adverse events among the 243 reported cardiac complications, post mRNA COVID-19 vaccination. Males with a median age of 21 years had the highest frequency of myocarditis. Almost three quarters (74.4%) of cases with myocarditis had received the BNT162b2 vaccine and 87.7% had received the second dose of the vaccine.[16]
Novel approaches to risk–benefit analysis such as Bayesian network models can integrate the latest global evidence with local factors to inform decision-making with regard to current vaccines in use.[17]
There are now at least 40 published papers questioning genetic mRNA vaccinations in children.[18]
As these genetic vaccines are still so new, no-one knows what the long-term outcome will be for those who suffer myocarditis following vaccination, or any other long-term risk for that matter. Although most children make a full recovery we don’t know if scaring of the heart occurred, which will induce early onset heart disease, even in those that return to full function.
Here are the latest CDC statistics regarding the death rate:
- 0.011% of the US population under 65 have died of COVID
- 0.005% of the US population under 55 have died of COVID
- 0.0009% of the US population under 35 have died of COVID
- 0.0002% of the US population under 25 have died of COVID
- 0.00008% of the US population under 15 have died of COVID
And as for the most “high risk” people?
- 0.23% of the US population over 65 have died of COVID.[19]
Omicron Related Hospitalizations – Do the Current Vaccines Help?
Earlier studies[20] confirmed a clear benefit at reducing the hospitalizations and death from Covid in those who were vaccinated, but Omicron is different and vaccines appear to be far less effective and whatever benefit vaccines may offer quickly diminishes – leaving us on a path of never-ending vaccines. Never before in history has something so quickly mutated with the capacity to out-wit vaccines.
Over the past 14 days, cases per 100,000 were higher in the fully vaccinated than in the unvaccinated. There is now emerging data that suggests Omicron is more contagious in the vaccinated than the unvaccinated.
Hospitalizations by Vaccination Status (As of January 16th, 2022) from Ontario Canada.
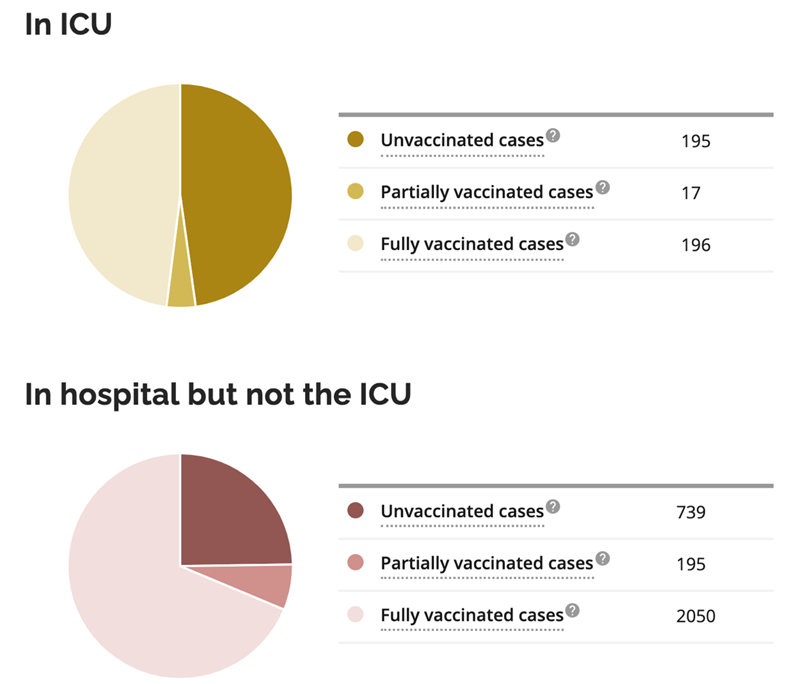
Omicron Cases by Vaccination Status (As of January 16th, 2022) from Ontario Canada.
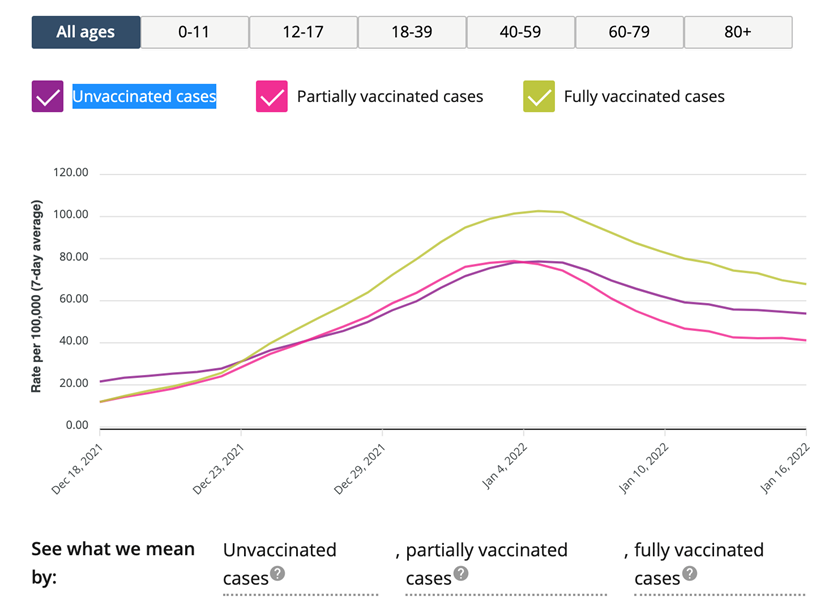
.[21]
According to new research from Western Cape Province, South Africa, outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave further suggest Omicron is less pathogenic with reduced risk of severe hospitalization or death compared to Delta.[22]
The more comorbidities, and the more severe the comorbidities, the greater the chances of death or severe adverse outcomes. Why aren’t we addressing the fact that our poor overall health status is the main reason we are in the situation we are in regarding sickness and death from COVID-19? Isn’t it time to ask if there might be something else we can do? What about nutrition and herbal medicine? Before the vaccine we heard about Vitamin D, Zinc and Quercetin; but since the vaccine there’s been no mention of these anymore. Could changes in our diet help? Certainly getting outside in the fresh air, which was so discouraged in the beginning – again, why? While there’s never been any data to support that approach, our national parks closed and people stayed inside because it’s what we were repeatedly told, even though the outdoors and good ventilation turned out to be very safe!
Researcher Blows the Whistle on Data Integrity Issues in Pfizer’s Vaccine Trial
Paul Thacker, a veteran investigational trial oversight manager with 15 years’ experience, in the November 2 issue of the British Medical Journal blew the whistle on data integrity in the Pfizer’s vaccine trial. What was uncovered was falsification of data, unblinding of patients, hiring individuals inadequately trained in vaccination, and delay in reporting and follow-up of adverse events in the critical Phase 3 of the vaccine trial.[23]
A Japanese biodistribution study for the Pfizer vaccine found that, in the 48 hours post-vaccination, vaccine particles had travelled to various tissues throughout the body and did not stay at the injection site, with high concentrations found at the liver, bone marrow, and ovaries.[24]
Recent emerging data suggests that effects related to inflammation and clotting may occur in any tissue in which the spike protein accumulates. In addition, studies in mice found that the spike protein is capable of crossing the blood-brain barrier. Thus, in humans it could potentially lead to neurological damage if it is not cleared from the body.[25]
The last credible thing Dr. Fauci said, was on February 25, 2020, when he told CBS News (CBS morning) the following: “You cannot avoid having infections since you cannot shut off the country from the rest of the world… Do not let the fear of the unknown…distort your evaluation of the risk of the pandemic to you relative to the risks that you face every day…do not yield to unreasonable fear.” From the day on his narrative and message took a dramatic shift.
Now it is clear to me that Dr Anthony Fauci has a tendency to see every health problem as being amenable to expensive pharmaceutical solutions, specifically vaccines, even when science supports other less intrusive, less expensive, and equally effective therapies that are available. Not a word about them – only vaccinate, stay home, wear a mask, social distance, and wash your hands multiple times a day.
On Wednesday January 19, 2022, British Prime Minister Boris Johnson says face masks will no longer be mandatory in public places and COVID-19 passports will be dropped for large events as infections level off in most parts of the country.[26]
The campaign by our government to prevent every possible infection of the SARS-CoV-2 virus regardless of the cost or scientific validation will have massive implications for decades to come, especially on the younger generation.
“You’ll be judged by three things; intelligence, energy and integrity. And if you don’t have the last one, don’t even bother with the first two. Integrity is up to you, you were not born with it and you can’t learn it in school.” – Miriam Palma Defensor-Santiago GCS QSC RMA (née Defensor; 15 June 1945 – 29 September 2016) was a Filipina academic, lawyer, judge, author, and politician who served in all three branches of the Philippine government: judicial, executive, and legislative
[1] https://www.nytimes.com/interactive/2021/us/covid-cases.html?name=styln-coronavirus®ion=TOP_BANNER&block=storyline_menu_recirc&action=click&pgtype=LegacyCollection&variant=0_Control&is_new=false
[2] https://www.riotimesonline.com/brazil-news/modern-day-censorship/covid-19-policy-leading-israeli-immunologist-writes-open-letter-it-is-time-to-admit-failure/
[3] León TM, Dorabawila V, Nelson L, et al. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May–November 2021. MMWR Morb Mortal Wkly Rep. ePub: 19 January 2022. DOI: http://dx.doi.org/10.15585/mmwr.mm7104e1
[4] Ledford, Heidi, ‘Killer’ immune cells still recognize Omicron variant, Nature 601, 307 (2022), doi: https://doi.org/10.1038/d41586-022-00063-0
[5] Keeton, R. et al. Preprint at medRxiv https://doi.org/10.1101/2021.12.26.21268380 (2021).
[6] Geurts van Kessel, C. H. et al. Preprint at medRxiv https://doi.org/10.1101/2021.12.27.21268416 (2021).
[7] Liu, J. et al. Preprint at medRxiv https://doi.org/10.1101/2022.01.02.22268634 (2022).
[8] Chen J, Wang R, Gilby NB, Wei GW. Omicron (B.1.1.529): Infectivity, vaccine breakthrough, and antibody resistance. ArXiv [Preprint]. 2021 Dec 1:arXiv:2112.01318v1. PMID: 34873578; PMCID: PMC8647651.
[9] Subramanian, S.V., Kumar, A. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. Eur J Epidemiol 36, 1237–1240 (2021). https://doi.org/10.1007/s10654-021-00808-7
[10] Friedman, Allon, January 13, 2022 Updated: January 13, 2022, https://www.theepochtimes.com/mkt_app/vaccine-mandates-unscientific-divisive-and-enormously-costly_4211742.html?v=ul
[11] Kostoff RN, Calina D, Kanduc D, Briggs MB, Vlachoyiannopoulos P, Svistunov AA, Tsatsakis A. Why are we vaccinating children against COVID-19? Toxicol Rep. 2021;8:1665-1684. doi: 10.1016/j.toxrep.2021.08.010. Epub 2021 Sep 14. Erratum in: Toxicol Rep. 2021;8:1981. PMID: 34540594; PMCID: PMC8437699.
[12] Ledford, Heidi, ‘Killer’ immune cells still recognize Omicron variant, Nature 601, 307 (2022), doi: https://doi.org/10.1038/d41586-022-00063-0
[13] Mevorach D, Anis E, Cedar N, Bromberg M, Haas EJ, Nadir E, Olsha-Castell S, Arad D, Hasin T, Levi N, Asleh R, Amir O, Meir K, Cohen D, Dichtiar R, Novick D, Hershkovitz Y, Dagan R, Leitersdorf I, Ben-Ami R, Miskin I, Saliba W, Muhsen K, Levi Y, Green MS, Keinan-Boker L, Alroy-Preis S. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med. 2021 Dec 2;385(23):2140-2149. doi: 10.1056/NEJMoa2109730. Epub 2021 Oct 6. PMID: 34614328; PMCID: PMC8531987.
[14] Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, Watkinson P, Khunti K, Harnden A, Coupland CAC, Channon KM, Mills NL, Sheikh A, Hippisley-Cox J. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. 2021 Dec 14. doi: 10.1038/s41591-021-01630-0. Epub ahead of print. PMID: 34907393.
[15] Husby A, Hansen JV, Fosbøl E, Thiesson EM, Madsen M, Thomsen RW, Sørensen HT, Andersen M, Wohlfahrt J, Gislason G, Torp-Pedersen C, Køber L, Hviid A. SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. BMJ. 2021 Dec 16;375:e068665. doi: 10.1136/bmj-2021-068665. PMID: 34916207; PMCID: PMC8683843.
[16] Fazlollahi A, Zahmatyar M, Noori M, Nejadghaderi SA, Sullman MJM, Shekarriz-Foumani R, Kolahi AA, Singh K, Safiri S. Cardiac complications following mRNA COVID-19 vaccines: A systematic review of case reports and case series. Rev Med Virol. 2021 Dec 17:e2318. doi: 10.1002/rmv.2318. Epub ahead of print. PMID: 34921468.
[17] Lau CL, Galea I. Risk-benefit analysis of COVID-19 vaccines – a neurological perspective. Nat Rev Neurol. 2021 Dec 20:1–2. doi: 10.1038/s41582-021-00606-5. Epub ahead of print. PMID: 34931027; PMCID: PMC8687148.
[18] Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections, Petra Zimmermann, Nigel Curtis
SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis, Tracy Beth Høeg, Allison Krug, Josh Stevenson, John Mandrola
Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units, Lara S. Shekerdemian, MD, MHA; Nabihah R. Mahmood, MD; Katie K. Wolfe, MD; et al.
Additional references regarding Covid-19 vaccine risks in children:
- State-Level Data on COVID-19 child mortality, American Academy of Pediatrics
- a. Deaths in Children and Young People in England following SARS-CoV-2 infection during the first pandemic year: a national study using linked mandatory child death reporting data, C. Smith, D. Odd, R Harwood, J. Ward, M. Linney, M. Clark, D. Hargreaves, SN Ladhani, E. Draper, PJ Davis, SE Kenny, E. Whittaker, K. Luyt, RM Viner, LK Fraser
- Risk factors for intensive care admission and death amongst children and young people admitted to hospital with COVID-19 and PIMS-TS in England during the first pandemic year, JL Ward, R. Harwood, C. Smith, S. Kenny, M. Clark, PJ Davis, ES Draper, D. Hargreaves, S. Ladhani, M. Linney, K. Luyt, S. Turner, E. Whittaker, LK Fraser, RM Viner
- Shedding of Infectious SARS-CoV-2 Despite Vaccination, Kasen K. Riemersma, Brittany E. Grogan, Amanda Kita-Yarbro, Peter J. Halfmann, Hannah E. Segaloff, Anna Kocharian, Kelsey R. Florek, Ryan Westergaard, Allen Bateman, Gunnar E. Jeppson, Yoshihiro Kawaoka, David H. O’Connor, Thomas C. Friedrich, Katarina M. Grande
- UK Government Recommendations on Vaccinating Children – Ages 12-15
- Comparison of children and young people admitted with SARS-CoV-2 across the UK in the first and second pandemic waves: prospective multicentre observational cohort study, Semple et al.
- Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum, Stuart P. Weisberg, Thomas J. Connors, Donna L. Farber
- Open Schools, Covid-19, and Child and Teacher Morbidity in Sweden, Jonas F. Ludvigsson, Lars Engerström, Charlotta Nordenhäll, Emma Larsson
- Transient Cardiac Injury in Adolescents Receiving the BNT162b2 mRNA Vaccine, Ori Snapiri, Chen Rosenberg Danziger, Nina Shirman, Avichai Weissbach, Alexander Lowenthal, Itay Ayalon, Dganit Adam, Havatzelet Yarden-Bilavsky, Efraim Bilavsky
- Myocarditis following COVID-19 mRNA vaccination, Saif Abu Mouch, Ariel Roguin, Elias Hellou, Amorina Ishai, Uri Shoshan, Lamis Mahamid, Marwan Zoabi, Marina Aisman, Nimrod Goldschmid, Noa Berar Yanay
- Myocarditis following COVID-19 vaccination, Albert, E., Aurigemma, G., Saucedo, J., Gerson, D. S.
- Acute Myocardial Infarction and Myocarditis following COVID-19 Vaccination, Aye, Y. N., Mai, A. S., Zhang, A., Lim, O. Z. H., Lin, N., Ng, C. H., . . . Chew, N. W. S.
- Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting, Barda, N., Dagan, N., Ben-Shlomo, Y., Kepten, E., Waxman, J., Ohana, R., . . . Balicer, R. D.
- COVID19 Vaccine for Adolescents. Concern about Myocarditis and Pericarditis, Calcaterra, G., Mehta, J. L., de Gregorio, C., Butera, G., Neroni, P., Fanos, V., Bassareo, P.
- Multisystem inflammatory syndrome in a male adolescent after his second Pfizer-BioNTech COVID-19 vaccine, Chai, Q., Nygaard, U., Schmidt, R. C., Zaremba, T., Moller, A. M., & Thorvig, C. M.
- Occurrence of acute infarct-like myocarditis following COVID-19 vaccination: just an accidental co-incidence or rather vaccination-associated autoimmune myocarditis?, Chamling, B., Vehof, V., Drakos, S., Weil, M., Stalling, P., Vahlhaus, C., . . . Yilmaz, A.
- Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far?, Das, B. B., Moskowitz, W. B., Taylor, M. B., Palmer, A.
- Biopsy-proven lymphocytic myocarditis following first mRNA COVID-19 vaccination in a 40-year-old male: case report, Ehrlich, P., Klingel, K., Ohlmann-Knafo, S., Huttinger, S., Sood, N., Pickuth, D., & Kindermann, M.
- Myocarditis should be considered in those with a troponin rise and unobstructed coronary arteries following Pfizer-BioNTech COVID-19 vaccination, Ioannou, A.
- Myocarditis Following COVID-19 Vaccination, Isaak, A., Feisst, A., & Luetkens, J. A.
- Myocarditis following COVID-19 vaccination, Kaul, R., Sreenivasan, J., Goel, A., Malik, A., Bandyopadhyay, D., Jin, C., . . . Panza, J. A.
- Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination, Kim, H. W., Jenista, E. R., Wendell, D. C., Azevedo, C. F., Campbell, M. J., Darty, S. N., . . . Kim, R. J.
- Cardiac Imaging of Acute Myocarditis Following COVID-19 mRNA Vaccination, Kim, I. C., Kim, H., Lee, H. J., Kim, J. Y., & Kim, J. Y.
- Why are we vaccinating children against COVID-19?, Kostoff, R. N., Calina, D., Kanduc, D., Briggs, M. B., Vlachoyiannopoulos, P., Svistunov, A. A., & Tsatsakis, A.
- Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination, Lee, E. J., Cines, D. B., Gernsheimer, T., Kessler, C., Michel, M., Tarantino, M. D., . . . Bussel, J. B.
- Myocarditis following COVID-19 vaccination – A case series, Levin, D., Shimon, G., Fadlon-Derai, M., Gershovitz, L., Shovali, A., Sebbag, A., . . . Gordon, B.
- Vaccine advisory committee must be more transparent about decisions, Mahase, E.
- COVID vaccines cut the risk of transmitting Delta – but not for long, Mallapaty, S.
- Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel, Mevorach, D., Anis, E., Cedar, N., Bromberg, M., Haas, E. J., Nadir, E., . . . Alroy-Preis, S.
- COVID-19 Vaccine-Induced Thrombosis and Thrombocytopenia: First Confirmed Case from India, Mishra, K., Barki, S., Pattanayak, S., Shyam, M., Sreen, A., Kumar, S., & Kotwal, J.
- Cardiovascular magnetic resonance findings in young adult patients with acute myocarditis following mRNA COVID-19 vaccination: a case series, Patel, Y. R., Louis, D. W., Atalay, M., Agarwal, S., & Shah, N. R.
- A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products, Rose, J., & McCullough, P. A.
- Transient Cardiac Injury in Adolescents Receiving the BNT162b2 mRNA COVID-19 Vaccine, Snapiri, O., Rosenberg Danziger, C., Shirman, N., Weissbach, A., Lowenthal, A., Ayalon, I., . . . Bilavsky, E.
- Myocarditis after Covid-19 Vaccination in a Large Health Care Organization, Witberg, G., Barda, N., Hoss, S., Richter, I., Wiessman, M., Aviv, Y., . . . Kornowski, R.
[19] Deaths involving coronavirus disease 2019 (COVID-19), pneumonia, and influenza reported to NCHS by sex, age group, and jurisdiction of occurrence; Jan. 12, 2022, https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-by-Sex-and-Age/9bhg-hcku
[20] Haas EJ, Angulo FJ, McLaughlin JM, Anis E, Singer SR, Khan F, Brooks N, Smaja M, Mircus G, Pan K, Southern J, Swerdlow DL, Jodar L, Levy Y, Alroy-Preis S. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021 May 15;397(10287):1819-1829. doi: 10.1016/S0140-6736(21)00947-8. Epub 2021 May 5. Erratum in: Lancet. 2021 Jul 17;398(10296):212. PMID: 33964222; PMCID: PMC8099315.
[21] https://covid-19.ontario.ca/data
[22] MaryAnn Davies, Reshma Kassanjee, et. al., Outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave compared with previous waves in the Western Cape Province, South Africa, medRxiv 2022.01.12.22269148;
[23] Thacker, Paul D. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial BMJ 2021; 375 doi: https://doi.org/10.1136/bmj.n2635 (Published 02 November 2021)Cite this as: BMJ 2021;375:n2635
[24] SARS-CoV-2 mRNA Vaccine (BNT162, PF-07302048) 2.6.4 Summary of pharmacokinetic study, PFIZER CONFIDENTIAL, https://www.naturalnews.com/files/Pfizer-bio-distribution-confidential-document-translated-to-english.pdf
[25] Rhea, E.M., Logsdon, A.F., Hansen, K.M. et al. The S1 protein of SARS-CoV-2 crosses the blood–brain barrier in mice. Nat Neurosci 24, 368–378 (2021). https://doi.org/10.1038/s41593-020-00771-8
[26] https://abcnews.go.com/Health/wireStory/uk-lifts-covid-restrictions-omicron-wave-peaked-82349201
What a thorough assessment. I feel like this article should be circulated far and wide, so more people can gain perspective. It’s objective, scientific, and at the same time, curious and humble. Thank you so much for your writings!
Amazing article! Thank you for this thorough research.
Thank you so much for offering this well thought out and researched perspective. I’ve been following your writing for a few months now and I am always eager to see what you’ve got to say next.
Blessings!