
Every parent in America who has a child in college is wondering about COVID-19 vaccine boosters for young people. What are the risks? What are the benefits?
This isn’t an easy question—deciding about COVID-19 vaccine boosters for young people can cause a lot of confusion.
So let me walk you through some of the issues you should consider, as well as some of the most recent peer-reviewed science about COVID-19 vaccine boosters for young people.
Background: mRNA Technology is Different from Conventional Vaccines
Most of us think of the new mRNA technology to protect against COVID-19 as a “vaccine” or a “jab.” But COVID-19 mRNA vaccines are not the same as simple conventional vaccines.
The mRNA vaccines are quite distinct from vaccines. They are more akin to other pharmaceutical drugs and should be therefore considered pharmaceuticals, not vaccines.
Here’s why: COVID-19 mRNA vaccines contain active SARS-CoV-2 S protein mRNA, which represents at the same time a prodrug and an active principle.
Although it might sound unconventional to define the content of a vaccine as a “prodrug,” the definition applies to these products.
As delivered, mRNAs theoretically act by triggering the production of distinct antigens that can distribute systemically throughout the body. This makes them radically different from conventional inactivated whole-virus vaccines and even protein-subunit nanoparticle vaccines. It’s important to keep this in mind when considering whether to accept COVID-19 vaccine boosters for young people.
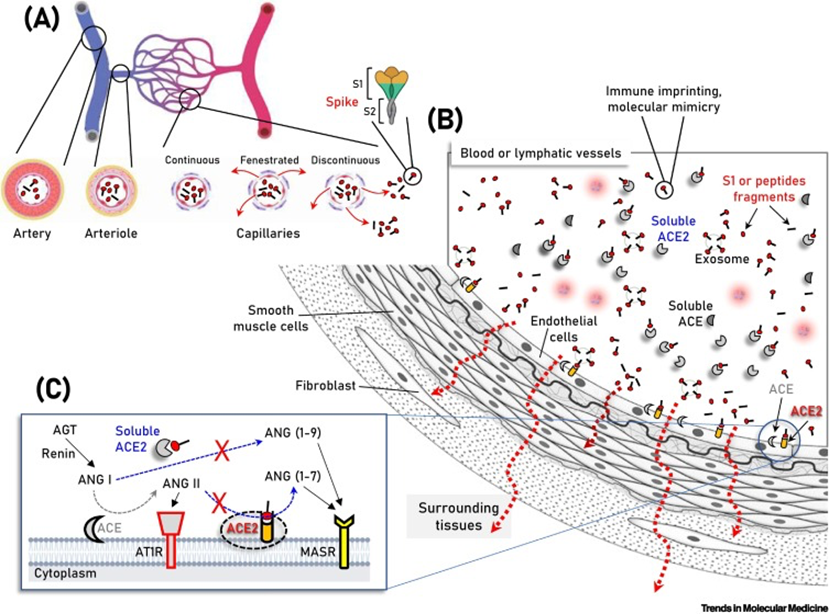
(A,B) Parallel to immune system activation, circulating S protein/subunits/peptide fragments (B) binding to ACE2 may occur not only to ACE2-expressing endothelial cells, but also in multiple cell types of the vasculature and surrounding tissues due to antigen diffusion (e.g., in fenestrated or discontinuous capillary beds) (A, red arrows). These series of molecular events are unlikely for any severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-related antigen in the absence of severe coronavirus disease 2019 (COVID-19), where SARS-CoV-2 is contained in the respiratory system. In (C) the two counteracting pathways of the renin–angiotensin system (RAS), namely the ‘conventional’ arm, that involves ACE which generates angiotensin II (ANG II) from angiotensin I (ANG I), and the ACE2 arm which hydrolyzes ANG II to generate angiotensin (1–7) [ANG (1–7)] or ANG I to generate angiotensin (1–9) [ANG (1–9)] are depicted. ANG II binding and activation of the ANG II type 1 receptor (AT1R) promotes inflammation, fibrotic remodeling, and vasoconstriction, whereas the ANG (1–7) and ANG (1–9) peptides binding to MAS receptor (MASR) activate antifibrotic, anti-inflammatory pathways and vasodilation. Additional modules of the RAS (i.e., renin and angiotensinogen, AGT) are also shown. Abbreviation: AT1R, angiotensin II type 1 receptor.[1]
Vaccine Boosters For Young People: Is There Cause for Concern?
At many universities in the United States, students (and staff) who have not received their third or fourth COVID-19 vaccines risk disenrollment if they do not want these boosters.
According to a December 2022 article in the Journal of Medical Ethics, however, these mandates are unethical. The scientists give five main reasons why COVID-19 vaccine boosters for young people should not be mandatory.
For one thing, there has not been a risk-benefit assessment of these vaccines for this age group, now that the virus has mutated and the Omicron variant is more prevalent.
For another, the booster shows “may result in a net harm to healthy young adults,” the scientists insist.
The third reason mandating COVID-19 vaccine boosters for young people is unethical is that the expected (known) harms of giving young adults these boosters may exceed any theoretical benefit to public health in general. In fact, the scientists call the benefits of the mRNA technology “modest” and note their “transient effectiveness … against transmission.”
Furthermore, they argue that young people who experience serious vaccine-related injuries (which include lifelong heart problems, an elevated risk of strokes, and sudden death) may not be fairly compensated after they are harmed. So, mandating these boosters violates the reciprocity principle.
Finally, in their assessment, booster shots may lead to even wider social harm instead of public health gains.[2]
More Boosters = Less Protection?
According to a January 2023 study by researchers in France,[3] the protection offered by a second mRNA booster was lower than the protection observed with the first booster.
At the same time, the same French study showed that previous infections offered high levels and long-lasting protection against symptomatic Omicron BA.2 or BA.4/5 infections.
FDA Vaccine Advisors Misled About Boosters
You may have seen in the news that vaccine advisors announced that they were “disappointed” and “angry.”
As reported by CNN, FDA advisors felt misled that scientists from the pharmaceutical industry and the government did not give them access to infection data in advance of meetings to discuss whether more injections should be authorized and made available to the public.
A preprint[4] showing that the boosters were not effective was posted online June 25, just three days before the FDA advisers met.
However, Michael Felberbaum, an FDA spokesperson, told CNN that “the FDA received the preprint less than a day prior to the advisory committee meeting.”
“The information was therefore not provided in an adequate timeframe for it to be included in the agency’s meeting materials, and generally the FDA only discusses data at advisory committee meetings that the agency has had the opportunity to substantively review.”[5]
Policymakers, public health scholars and bioethicists have argued both for and against COVID-19 vaccine mandates.
The strongest argument made by proponents of vaccine mandates is based on the harm principle: insofar as vaccines prevent transmission and thereby reduce harm to others, restrictions on individual freedom are viewed as more ethically justifiable.[6]
However, a reduction in risk to others (especially if this is a small or temporary effect) might not alone be sufficient to justify a booster mandate in young people.
Others[7],[8] have argued that to be ethical, mandates require four conditions:
- That the disease be a grave public health threat;
- That there is a safe and effective vaccine;
- That mandatory vaccination has a superior cost/benefit profile in comparison to other alternatives;
- and that the level of coercion is proportionate to the threat.
COVID-19 vaccine boosters for young people do not satisfy these criteria.
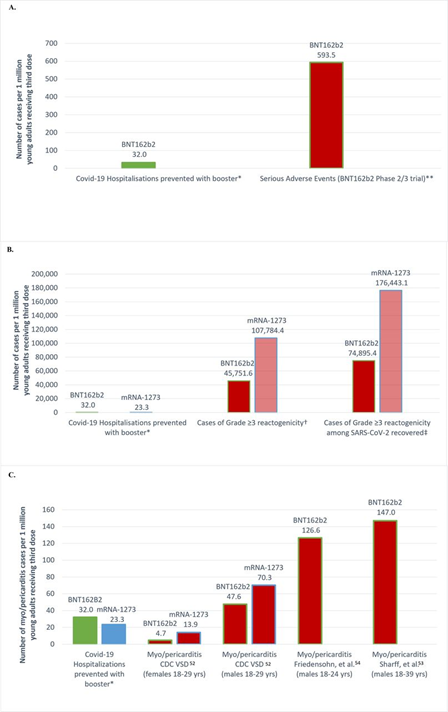
At the same time, age and gender are prominent risk factors for vaccine-associated reactogenicity.[9] Moreover, serious adverse events, such as myocarditis, is much, much more common in young people—especially men.[10],[11],[12],[13]
Cohort Study of 23 Million People
A study of 23.1 million people across four Scandinavian countries showed the risk of myocarditis after the first and second doses of SARS-CoV-2 mRNA injections was highest in young males aged 16 to 24 years after the second dose.
This risk must “be balanced against the benefits of protecting against severe COVID-19 disease,” the scientists rightly concluded.[14]
Mandates Cause Harm
Mandates cause social harm. Forced vaccination, despite controversy among experts, have no updated risk-benefit analyses based on currently circulating variants, is misguided at best and unethical, and perhaps even felonious.
There has been a profound lack of transparency in scientific and regulatory policymaking, which is a huge cause for concern.[15]
Bias in Reporting Vaccine Efficacy
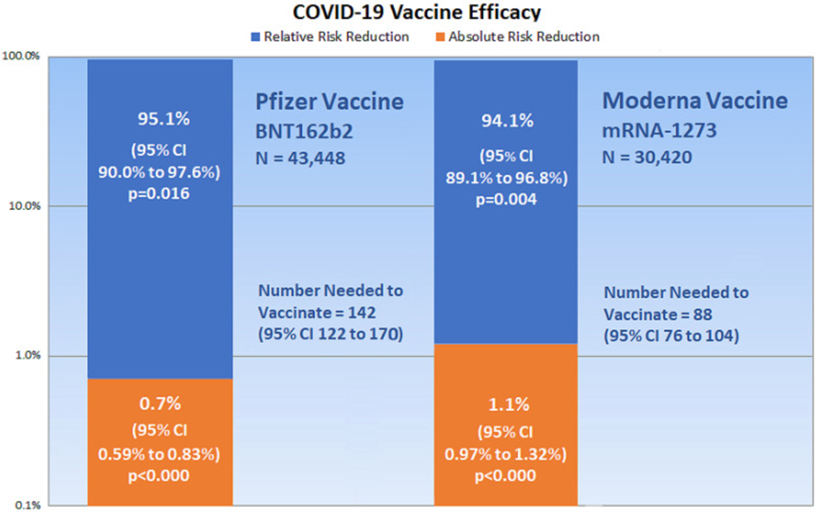
The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that falsely inflates evidence of vaccine efficacy.[17] So even when the vaccines are not effective, the public is wrongly led to believe that they are.
Let me say a little more about this: Relative Risk Rate (RRR) is the ratio of attack rates with and without vaccination, which has been reported as 95% and 94.5% for Pfizer/BioNTech Vaccine and Moderna Vaccine, respectively.[18]
However, measuring efficacy only by RRR introduces biases and makes it almost impossible to get a real sense of vaccine efficacy. Vaccine efficacy must be assessed based on the risk of becoming infected with the SARS-CoV-2, which varies with time and populations under study.
Absolute Risk Rate (ARR), on the other hand, is the difference between attack rates among people who have had the vaccines versus those who have not.
These numbers are pitiful. The ARR for Pfizer/BioNTech Vaccine is 0.7% and for Moderna Vaccine is 1.1%. You can see that these are meager values compared to relative risk rates.[19]
Adverse Events Following COVID-19 Vaccination: What’s Going On?
There is no longer any controversy about the reactogenicity of these injections. At least not in the scientific literature.
In fact, we have over a thousand peer-reviewed articles now showing evidence of harm.
And this harm, when it happens to young people who are not at risk of severe COVID-19 infection, is especially disturbing.
I always like to ask why? What’s going wrong? What underlying biochemical mechanisms are at work that are causing so many adverse outcomes?
Might it have something to do with the vaccine ingredients?
In a 2022 study, a team of nine scientists based in Greece argued that both the lipid nanoparticles and the spike proteins may be to blame.
“Adverse effects following vaccination have been noted which may relate to a proinflammatory action of the lipid nanoparticles used or the delivered mRNA (i.e., the vaccine formulation),” the scientists explain, “as well as to the unique nature, expression pattern, binding profile, and proinflammatory effects of the produced antigens—spike (S) protein and/or its subunits/peptide fragments—in human tissues or organs.”[20]
Spike Protein Highly Problematic
A comprehensive review of the literature recently discussed the role of COVID-19- mRNA-vaccine-induced S protein in adverse effects following vaccination.
This paper, co-authored by two Italian scientists, showed that the production of S protein induced by COVID-19 mRNA vaccines may well compare to the estimated production during SARS-CoV-2 infection.
As the scientists explain:
“Based on these premises, a major explanation of adverse effects following COVID-19 vaccination could well be that mRNA vaccines induce in selected individuals excessive production of S protein, for too long and/or in inappropriate tissues and organs, and this occurrence is at present unpredictable, since systemic biodistribution and disposition of the COVID-19 mRNA vaccine has so far never been considered an issue, and as a consequence it has never been studied as it would have actually deserved.”
They continue: “Remarkably, the inadequate understanding of how to target specific organs and cells for protein expression is well-acknowledged as one of the major limitations of mRNA gene therapy; however, for mRNA vaccines, it has been so far ignored.”[21]
When considering COVID-19 vaccine boosters for young people, a risk-benefit analysis based on recent studies shows that the boosters are not effective, not necessary, and may cause myriad harms.
“Truth is incontrovertible. Panic may resent it. Ignorance may deride it. Malice may distort it. But there it is.” ~WINSTON CHURCHILL
About the author: Donnie Yance is an internationally recognized health advocate and the author of Adaptogens in Medical Herbalism.
[1] Trougakos IP, Terpos E, Alexopoulos H, Politou M, Paraskevis D, Scorilas A, Kastritis E, Andreakos E, Dimopoulos MA. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Trends Mol Med. 2022 Jul;28(7):542-554. doi: 10.1016/j.molmed.2022.04.007. Epub 2022 Apr 21.
[2] Bardosh K, Krug A, Jamrozik E, et al COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities
Journal of Medical Ethics Published Online First: 05 December 2022. doi: 10.1136/jme-2022-108449
[3] Cynthia Tamandjou, Vincent Auvigne, Justine Schaeffer, Sophie Vaux, Isabelle Parent du Châtelet, Effectiveness of second booster compared to first booster and protection conferred by previous SARS CoV-2 infection against symptomatic Omicron BA.2 and BA.4/5 in France medRxiv 2023.01.11.23284137; doi: https://doi.org/10.1101/2023.01.11.23284137
[4] Chalkias S, Harper C, Vrbicky K, Walsh SR, Essink B, Brosz A, McGhee N, Tomassini JE, Chen X, Chang Y, Sutherland A, Montefiori DC, Girard B, Edwards DK, Feng J, Zhou H, Baden LR, Miller JM, Das R. A Bivalent Omicron-Containing Booster Vaccine against Covid-19. N Engl J Med. 2022 Oct 6;387(14):1279-1291. doi: 10.1056/NEJMoa2208343. Epub 2022 Sep 16. PMID: 36112399; PMCID: PMC9511634.
[5] Elizabeth Cohen, Naomi Thomas, FDA vaccine advisers ‘disappointed’ and ‘angry’ that early data about new Covid-19 booster shot wasn’t presented for review last year | CNN, January 11, 2023, https://synopsi.medpagetoday.com/article/210134/fda-vaccine-advisers-disappointed-and-angry-that-early-data-about-new?xid=nl_synopsi_2023-01-22&mh=d458aaaea88a68d8894f442010dd1cd1
[6] World Health Organization. COVID-19 and mandatory vaccination: ethical considerations: policy brief, 2022. Available: https://www.who.int/publications/i/ item/WHO-2019-nCoV-Policy-brief-Mandatory-vaccination-2022.1 [Accessed 20 Aug 2022].
[7] Savulescu J. Good reasons to vaccinate: mandatory or payment for risk? J Med Ethics 2021;47(2):78–85.
[8] Giubilini A, Savulescu J, Wilkinson D. COVID-19 vaccine: vaccinate the young to protect the old? J Law Biosci 2020;7(1).
[9] Ughi N, Del Gaudio F, Dicuonzo A, et al. Host factors and history of SARS-CoV-2 infection impact the reactogenicity of BNT162b2 mRNA vaccine: results from a cross-sectional survey on 7,014 workers in healthcare. Eur Rev Med Pharmacol Sci 2021;25(24):7985–96.
[10] Karlstad Øystein, Hovi P, Husby A, et al. SARS-CoV-2 vaccination and myocarditis in a Nordic cohort study of 23 million residents. JAMA Cardiol 2022;7(6):600–12.
[11] Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, Watkinson P, Khunti K, Harnden A, Coupland CAC, Channon KM, Mills NL, Sheikh A, Hippisley-Cox J. Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation. 2022 Sep 6;146(10):743-754. doi: 10.1161/CIRCULATIONAHA.122.059970. Epub 2022 Aug 22. PMID: 35993236; PMCID: PMC9439633.
[12] Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, Watkinson P, Khunti K, Harnden A, Coupland CAC, Channon KM, Mills NL, Sheikh A, Hippisley-Cox J. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. 2022 Feb;28(2):410-422. doi: 10.1038/s41591-021-01630-0. Epub 2021 Dec 14. PMID: 34907393; PMCID: PMC8863574.
[13] Bots SH, Riera-Arnau J, Belitser SV, Messina D, Aragón M, Alsina E, Douglas IJ, Durán CE, García-Poza P, Gini R, Herings RMC, Huerta C, Sisay MM, Martín-Pérez M, Martin I, Overbeek JA, Paoletti O, Pallejà-Millán M, Schultze A, Souverein P, Swart KMA, Villalobos F, Klungel OH, Sturkenboom MCJM. Myocarditis and pericarditis associated with SARS-CoV-2 vaccines: A population-based descriptive cohort and a nested self-controlled risk interval study using electronic health care data from four European countries. Front Pharmacol. 2022 Nov 24;13:1038043. doi: 10.3389/fphar.2022.1038043. PMID: 36506571; PMCID: PMC9730238.
[14] Karlstad Ø, Hovi P, Husby A, et al. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiol. 2022;7(6):600–612. doi:10.1001/jamacardio.2022.0583
[15] Oliver S. Updates to the evidence to recommendation framework: Pfizer-BioNTech and Moderna COVID-19 vaccine booster doses. ACIP meeting. November 19, 2021. (slides 26, 29, 30, 31, 37), 2021. Available: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-11-19/06-COVID-Oliver-508.pdf [Accessed 28 Mar 2022].
[16] Ali T, Mujawar S, Sowmya AV, Saldanha D, Chaudhury S. Dangers of mRNA vaccines. Ind Psychiatry J. 2021 Oct;30(Suppl 1):S291-S293. doi: 10.4103/0972-6748.328833. Epub 2021 Oct 22. PMID: 34908713; PMCID: PMC8611574.
[17] Brown RB. Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Medicina (Kaunas). 2021 Feb 26;57(3):199. doi: 10.3390/medicina57030199. PMID: 33652582; PMCID: PMC7996517.
[18] Meo SA, Bukhari IA, Akram J, Meo AS, Klonoff DC. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and moderna vaccines. Eur Rev Med Pharmacol Sci. 2021;25:1663–9
[19] Brown RB. Outcome reporting bias in COVID-19 mRNA vaccine clinical trials. Medicina (Kaunas) 2021;57:199.
[20] Trougakos IP, Terpos E, Alexopoulos H, Politou M, Paraskevis D, Scorilas A, Kastritis E, Andreakos E, Dimopoulos MA. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Trends Mol Med. 2022 Jul;28(7):542-554. doi: 10.1016/j.molmed.2022.04.007. Epub 2022 Apr 21.
[21] Cosentino M, Marino F. Understanding the Pharmacology of COVID-19 mRNA Vaccines: Playing Dice with the Spike? Int J Mol Sci. 2022 Sep 17;23(18):10881. doi: 10.3390/ijms231810881.
I’m so glad to have found your website and all this wonderful information! I’m a fellow herbalist that has had the pleasure of hearing and seeing your talks throughout the years. I believe one of those talks was at the HerbFest hosted by Frontier Herbs years ago. Thank you so much Donnie!!
Important information! We need to acknowledge, apply and advocate for what we have learned.